
By: Lauren Harnois, Alex Muller, Anna Kuruc, and Urvinder Kaur
When posed the question if airway clearance and lung expansion techniques were relevant to infants we originally believed they were. After reading the available research, our opinion has changed. In all of the articles we found, infants who received chest physiotherapy (CPT) had no significant difference in outcomes compared to infants who received traditional care. The main techniques to implement chest physiotherapy in infants are through positioning, percussion, and vibration. The theory behind these therapies is that it loosens and moves the secretions centrally in the lungs to be cleared out. There are also many potential adverse side effects that are associated with CPT that make it a poor therapy choice for infants.1 The significant risks involved with lung expansion therapies also make them an unpopular treatment choice for infants.
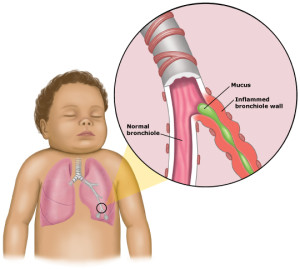
In a review of twelve randomized controlled trials, researchers looked to see if CPT techniques reduced the severity of bronchiolitis in infants from zero to twenty-four months old. CPT involved percussion and vibration. A reduction in severity was defined as a decreased length of hospital stay, need for oxygen, bronchodilator and steroid use, and time to recovery. No significant difference was found between the control group and infants who received CPT.1
In a similar study, four hundred and ninety six infants who had acute bronchiolitis were randomly selected to receive CPT in an attempt to determine if CPT was beneficial. CPT in this study involved an increased exhalation technique and assisted cough. Effectiveness of CPT was measured by time to recovery, antibiotic use, side effects, and ICU admissions. Time to recovery was 2.31 days in the control group, and 2.02 days in the CPT group, but this difference was not found to be statistically significant. The main difference in outcomes between the two groups was the occurrence of transient respiratory destabilization and vomiting, which occurred more in the CPT group.2
An additional study looked at one hundred and six infants who were mechanically ventilated with respiratory disease to determine if CPT (percussion and vibrations) changed their clinical course. Researchers in this study compared oxygen use, length of hospital stay, and weight of secretions cleared between the control and CPT group. Again, no significant difference was found between the two groups.3
Comparing the results of all three studies, it can be suggested that CPT in infants is not a beneficial therapy. There was no difference between recovery times, length of hospital stays, or the amount of secretions cleared. Not only was there no benefit to CPT, but there is also an increased risk of adverse side effects occurring. A few of the adverse effects that can occur include: rib fractures, hypoxemia, intraventricular hemorrhage, and bradycardia. Rib fractures can occur during percussion because the infant’s chest wall is thin and the ribs are more cartilaginous. Intraventricular hemorrhage is a risk because infants are unable to regulate cerebral blood flow, and the many positions involved in CPT can cause an increased intracranial pressure and rupture of blood vessels. Hypoxemia and bradycardia result from handling the infant. Careful monitoring must be carried out in infants who do receive CPT to avoid these effects.4
Common forms of hyperinflation therapy include incentive spirometry (IS) and intermittent positive pressure breathing (IPPB). Very little research was found on lung expansion techniques in infants, because IS is not a feasible therapy for infants for obvious reasons (e.g., IS requires coordination and the ability to follow instructions), and IPPB is not a standard treatment option for them. IPPB is a hyperinflation therapy, commonly used to treat atelectasis and improve lung function. IPPB is reserved for older children and adults because of the significant hazards that are associated with the therapy. Some of the hazards include: volutrauma, pneumothorax, hemoptysis, decreased venous return, and bronchospasm. These risks can be deadly to infants, so ultimately the risks outweigh the benefits.4
In conclusion, CPT is a time consuming therapy that shows no significant benefit, and an increased risk for adverse outcomes in infants. Based on the research available, CPT should be omitted from routine care of infants with respiratory disease. Hyperinflation techniques are also not a good treatment choice for infants. There is a significant amount of risk involved with therapies such as IPPB, and the risk is not worth the benefit. Further studies need to be conducted to determine what airway clearance techniques and hyperinflation techniques (if any) have a positive effect on infant outcomes.
References
- Roque i Figuls M, Gine-Garriga M, Granados Rugeles C, Perrotta C, Vilaro J. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev 2016;2:CD004873.
- Gajdos V, Katsahian S, Beydon N, Abadie V, de Pontual L, Larrar S, et al. Effectiveness of chest physiotherapy in infants hospitalized with acute bronchiolitis: a multicenter, randomized, controlled trial. PLoS Med 2010;7(9):e1000345.
- Hough JL, Flenady V, Johnston L, Woodgate PG. Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support. Cochrane Database Syst Rev 2008;(3):CD006445. doi(3):CD006445.
- Walsh BK. Neonatal and Pediatric Respiratory Care. In: 4th edition. St, Louis, Missouri:Saunders; 2015:203.
